Download presentation
Presentation is loading. Please wait.

1
Based on an original presentation by Hing Har Lo, MD Chair, Radiology/Nuclear Medicine hlo@vcom.edu Dr. Januchowski 2012

2
Name the different Imaging modalities available for the OB/GYN patient Compare and contrast the modalities available Know the different indications for imaging of the OB/GYN patient Choose the most appropriate modality based on the clinical presentation and desired results Recognize common OB/GYN Clinical presentations on imaging

3
X-Ray Ultrasound (US) Most important imaging Computerized Tomography (CT) Magnetic Resonance Imaging (MRI)
 Most important imaging Computerized Tomography (CT) Magnetic Resonance Imaging (MRI) ")
5
a low-dose, low voltage x-ray exam of the The results are recorded on x-ray film or directly into a computer (digital) Lump or mass Calcifications: Macrocalcifications are large calcium deposits often caused by aging. These usually are not a sign of cancer. Microcalcifications are tiny specks of calcium that may be found in an area of rapidly dividing cells. Distortion Still the diagnostic tool for detecting breast cancer Recommend screening after 40 yo

6
MLO of a fatty breast Small carcinoma Dense breast CC (cranial caudate) Analog Digital
 Analog Digital")
7
Performed with observing with fluoroscopy Injecting iodinated contrast via the catheter in the cervix/uterus/fallopian tubes Infertility evaluation Repeated miscarriages Monitor tubal patency after surgery A: right tube, B: uterine cavity, C: left tube, D: catheter with balloon tip Spillage into pelvis

8
Need a full bladder for an acoustic window. Sagittal scan through the long axis of uterus

9
Need a empty bladder. Adapted from: Danforth's Obstetrics and Gynecology 9 th Edition A transducer in vaginal probe inserted.

10
Sending high frequency sound waves in the transducer, Produce “echoes” of varying intensities received by the transducer ) Hyperechoic (echogenic) Isoechoic Isoechoic Hypoechoic Anechoic Echoes
 Hyperechoic (echogenic) Isoechoic Isoechoic Hypoechoic Anechoic Echoes")
11
Acoustic shadowing Acoustic enhancement Acoustic enhancement Calcification www.ultrasound-images.com/uterus.htm

12
Uses x-ray beams & detector arrays Attenuation, density Barium in small bowel uterus air in colon

13
Strong magnetic field Radio frequency (RF) Signal
 Signal")
14
Which of the following modalities would expose the patient to the largest amount of radiation? Ultrasound of the pelvis MRI of the abdomen Hysterosalpingogram Abdominal flat plate Mammography SEE NOTES FOR ANSWER

15
Obstetrics Growth & development Fetal well-being Abnormal Gynecology Anomalies Inflammatory Neoplastic Other

16
Gestational sac visible ~ 4 weeks Yolk sac visible ~ 4 -5 weeks Embryo visible ~ 5 - 6 weeks Heartbeat ~ 5 - 6 weeks Preembryonic period (conception to 5 menstrual wks); Embryonic period, during which time organogenesis is the major activity (4 to 9 menstrual weeks); Early developmental or fetal period, during which time the fetus continues to grow.
; Embryonic period, during which time organogenesis is the major activity (4 to 9 menstrual weeks); Early developmental or fetal period, during which time the fetus continues to grow.")
17
A gestational sac appears as a double ring that is comprised of the decidua capsularis and the decidua parietalis. The sac should be seen when the β human chorionic gonadotropin (hCG) is between 1,000 and 2,000 mIU/mL. Once identified, the sac diameter should grow by an average of 1 mm per day Yolk sac
 is between 1,000 and 2,000 mIU/mL. Once identified, the sac diameter should grow by an average of 1 mm per day Yolk sac.")
18
Crown-rump length

19
Biparietal diameter (BPD) Head circumference (HC) Abdominal circumference (AC) Femur length (FL)
 Head circumference (HC) Abdominal circumference (AC) Femur length (FL)")
20
Gestational age Fetal weight Fetal growth

21
CRL: +/- 3-4 days BPD, HC, AC, FL 14-22 wks GA: +/- 1 wk 23-30 wks GA: +/- 2 wks > 30 wks GA: +/- 3 wks

22
Use US age < 22 weeks Use menstrual age > 22 weeks Do not alter GA by US after 22 weeks Unless late 1 st prenatal evaluation Unsure of LMP

23
There are more than 40 formulas in the literature for estimated fetal weight (EFW). The Hadlock formula, which is incorporated into most North American ultrasound machine software packages, utilizes four variables: the BPD, HC, AC, and FL. Not highly accurate, but.. Benefits Growth rate evaluation Preterm labor

24
454gm=1lb Amniotic Fluid Index

26
Evaluate for fetal distress (hypoxia) Use Fetal Biophysical Profile
 Use Fetal Biophysical Profile")
27
1. Heart rate reactivity (non-stress test) 2 or more episodes of acceleration of ≥ 15 bmp and of >15 s associated with fetal movement within 20 min 2. Sufficient amniotic fluid: 1 or more pockets of fluid measuring ≥ 2 cm in vertical axis 3. Fetal tone :1 or more episodes of active extension with return to flexion of fetal limb(s) or trunk (opening and closing of hand considered normal tone) 4. Fetal movement 5. Fetal breathing Attempt to identify fetal distress (hypoxia) Analogous to neonatal Apgar score Points for each: 2 or 0 Normal: 8 – 10 points Suspicious: 6 points Abnormal: < 6 points http://www.emedicine.com/radio/topic758.htm
 2 or more episodes of acceleration of ≥ 15 bmp and of >15 s associated with fetal movement within 20 min 2. Sufficient amniotic fluid: 1 or more pockets of fluid measuring ≥ 2 cm in vertical axis 3. Fetal tone :1 or more episodes of active extension with return to flexion of fetal limb(s) or trunk (opening and closing of hand considered normal tone) 4. Fetal movement 5. Fetal breathing Attempt to identify fetal distress (hypoxia) Analogous to neonatal Apgar score Points for each: 2 or 0 Normal: 8 – 10 points Suspicious: 6 points Abnormal: < 6 points")
28
Tone 2 pts Breathing 2 pts Movement 2 pts Amniotic fluid 2 pts

29
Identify intrauterine pregnancy: Gestational sac Yolk sac Embryo Middleton: Ultrasound - The Requisites, 2nd ed. 2004 Mosby Embryonic heart rate: Should not be less than 90-100 bpm. Normally 120-180 bpm after 8 weeks Bradycardia often associated with miscarriage Less than 90 bpm at 5-6 weeks Less than 120 bpm after 8 weeks By 6 weeks: Should see heart beat by transvaginal US. If no embryo, or embryo without heartbeat – likelihood of miscarriage. By 7+ weeks: Normal heart beat implies high likelihood of progression to term.

30
Under ideal situations, at what gestational age would the gestational sac be visible on transvaginal pelvic ultrasound? 4 weeks 5 weeks 6 weeks 7 weeks ANSWER ANSWER

31
At what range would crown-rump length be the best measurement for the estimation of fetal gestational age? 0-5 weeks 6-14 weeks 15-22 weeks 22-30 weeks ANSWER ANSWER

32
Which of the following factors would be a part of the biophysical profile ultrasound to assess fetal well being? Umbilical artery flow rate Femur length Abdominal circumference Fetal heart rate Fetal lie ANSWER ANSWER

34
Relative risk of preterm delivery increases as cervical length decreases. Normal > 25mm. 25 mm optimal cutoff for predicting preterm delivery at all gestational ages. 40mm

35
Usually due to placental insufficiency Increased risk for fetal distress

36
Usually due to placental insufficiency Placenta requires adequate blood flow From Danforth's Obstetrics and Gynecology 9 th Edition Normal Uterine Artery WaveformAbnormal Uterine Artery Waveform Doppler Ultrasound

38
Doppler US ROI is at cardiac position of the fetus

39
Hydrocephalus Encephalocele Anencephaly Adapted from Gabbe: Obstetrics: Normal and Problem Pregnancies, 5th ed. 2007

40
Danforth's Obstetrics and Gynecology 9 th Edition

41
Adapted from: Danforth's Obstetrics and Gynecology 9 th Edition

42
Adapted from: http://www.uhrad.com/mamarc/mam030.htm Gestational trophoblastic disease Placental neopastic process Usually benign

43
Find IUP by transvaginal US Note: Heterotopic pregnancy 1 in 4000 – 30000 Discriminatory β hCG level Point at which all IUPs should be visible on TVUS Third International Standard: ~1500-2000 mIU/mL Exception: multiple gestations US visualization of extrauterine gestational sac

44
Free fluid Uterus Free Fluid Ectopic GS Adapted from Gabbe: Obstetrics: Normal and Problem Pregnancies, 5th ed. 2007

45
Which of the following ultrasound findings would indicate that a patient may be at higher risk for preterm labor? Fetal weight at <5 th percentile Uterine wall hypertrophy Cervical length < 25 mm Marginal placental previa SEE NOTES FOR ANSWER

46
Clinical presentations Obstetrics Growth & development Fetal well-being Abnormal Ectopic Gynecology Uterine Anomalies Inflammatory Neoplastic Miscellaneous

47
radiology.rsnajnls.org Infertility Miscarriage Ectopic pregnancy

48
imaging.consult.com Danforth's Obstetrics and Gynecology 9 th Edition Transverse US: Bicornuate or septated uterus Coronal MRI: Bicornuate Uterus

49
Berek & Novak's Gynecology Left adnexa: Tubo-ovarian abscess

50
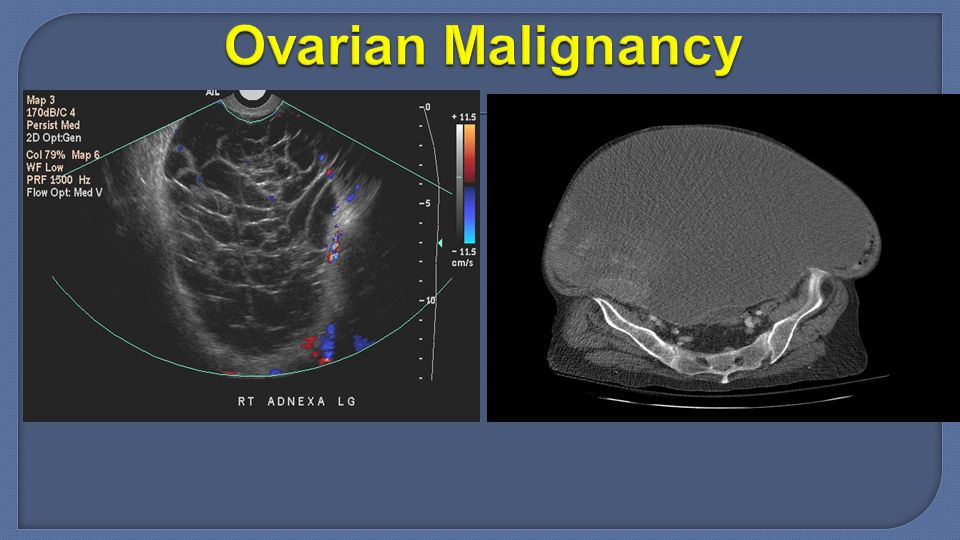
Benign Leiomyomata (fibroids) Ovarian teratoma (dermoid) Malignant Uterine Ovarian
 Ovarian teratoma (dermoid) Malignant Uterine Ovarian")
51
Berek & Novak's Gynecology http://fibroidshouston.com/uterine-fibrosis-diagnosed.htm http://www.fibroidspecialist.co.uk/fibroids.htm Ultrasound MRI NOTE: Most fibroids will be seen with smooth edges on ultrasound

52
Ultrasound CT Tooth

53
http://www.mghradrounds.org/index.php?src=gendocs&link=2005_april Normal endometrial thickness < 5mm post-menopausal

55
Functional (physiologic) Follicular Corpus luteum cyst Often acute abdominal pain due to: Large size Torsion Rupture Hemorrhage
 Follicular Corpus luteum cyst Often acute abdominal pain due to: Large size Torsion Rupture Hemorrhage")
56
Follicular Cyst Corpus Luteum Cyst Hemorrhagic Cyst

57
Normal right ovary Torsion left ovary Post-op left ovary

58
Normal ovary PCOS “String-of-pearls” sign

59
http://www.learningradiology.com/ Pelvic congestion is becoming increasingly recognised as a cause of chronic pelvic pain. It is associated with pelvic varicosities, increased blood flow

60
An ultrasound is done on a postmenopausal female for evaluation of vaginal bleeding. Which of the following findings would be most indicative of endometrial cancer in this patient? String of pearls sign Endometrial thickness of 7 mm Mass with smooth edges noted on ultrasound Increased blood flow to the pelvis ANSWER ANSWER

61
The End !

Similar presentations





 of less than 5 mm located within the thickened,>")






, Javam M. (B.Sc), Ahmadi F. (MD)>")





 Transducer placed on patient’s body Sound waves echo.>")




