Download presentation
Presentation is loading. Please wait.

1
Attribution: Kim Eagle, M.D., 2012 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution–Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/ We have reviewed this material in accordance with U.S. Copyright Law and have tried to maximize your ability to use, share, and adapt it. The citation key on the following slide provides information about how you may share and adapt this material. Copyright holders of content included in this material should contact open.michigan@umich.edu with any questions, corrections, or clarification regarding the use of content. For more information about how to cite these materials visit http://open.umich.edu/education/about/terms-of-use. Any medical information in this material is intended to inform and educate and is not a tool for self-diagnosis or a replacement for medical evaluation, advice, diagnosis or treatment by a healthcare professional. Please speak to your physician if you have questions about your medical condition. Viewer discretion is advised: Some medical content is graphic and may not be suitable for all viewers.

2
Attribution Key for more information see: http://open.umich.edu/wiki/AttributionPolicy Use + Share + Adapt Make Your Own Assessment Creative Commons – Attribution License Creative Commons – Attribution Share Alike License Creative Commons – Attribution Noncommercial License Creative Commons – Attribution Noncommercial Share Alike License GNU – Free Documentation License Creative Commons – Zero Waiver Public Domain – Ineligible: Works that are ineligible for copyright protection in the U.S. (17 USC § 102(b)) *laws in your jurisdiction may differ Public Domain – Expired: Works that are no longer protected due to an expired copyright term. Public Domain – Government: Works that are produced by the U.S. Government. (17 USC § 105) Public Domain – Self Dedicated: Works that a copyright holder has dedicated to the public domain. Fair Use: Use of works that is determined to be Fair consistent with the U.S. Copyright Act. (17 USC § 107) *laws in your jurisdiction may differ Our determination DOES NOT mean that all uses of this 3rd-party content are Fair Uses and we DO NOT guarantee that your use of the content is Fair. To use this content you should do your own independent analysis to determine whether or not your use will be Fair. { Content the copyright holder, author, or law permits you to use, share and adapt. } { Content Open.Michigan believes can be used, shared, and adapted because it is ineligible for copyright. } { Content Open.Michigan has used under a Fair Use determination. }
) *laws in your jurisdiction may differ Public Domain – Expired: Works that are no longer protected due to an expired copyright term. Public Domain – Government: Works that are produced by the U.S. Government. (17 USC § 105) Public Domain – Self Dedicated: Works that a copyright holder has dedicated to the public domain. Fair Use: Use of works that is determined to be Fair consistent with the U.S. Copyright Act. (17 USC § 107) *laws in your jurisdiction may differ Our determination DOES NOT mean that all uses of this 3rd-party content are Fair Uses and we DO NOT guarantee that your use of the content is Fair. To use this content you should do your own independent analysis to determine whether or not your use will be Fair. { Content the copyright holder, author, or law permits you to use, share and adapt. } { Content Open.Michigan believes can be used, shared, and adapted because it is ineligible for copyright. } { Content Open.Michigan has used under a Fair Use determination. }.")
3
Kim A. Eagle, M.D. University of Michigan Cardiovascular Center Acute Coronary Syndromes (ACS) Cardiovascular Sequence Fall 2012
 Cardiovascular Sequence Fall")
4
Kim A. Eagle, MD Director University of Michigan Cardiovascular Center Grants: NIH, Hewlett Foundation, Mardigian Foundation, Varbedian Fund, GORE Consultant: NIH NHLBI

5
Acute Coronary Syndromes Key Words: ST elevation MI, non-STE, ACS, cardiac biomarkers, treatment of ACS, mechanical complications of MI Objectives: 1.To learn how the admission ECG dictates early therapy for ACS. 2.To learn how to use cardiac biomarkers to diagnose ACS. 3.To become familiar with strategies for treatment in ACS. 4.To become familiar with mechanical complications of ACS.

6
Lecture Outline Pathogenesis of ACS Clinical features of ACS Treatment of ACS Complications Post ACS risk stratification

7
Pathogenesis of ACS Normal hemostasis Endogenous antithrombotic mechanisms Pathogenesis of coronary thrombosis Nonatherosclerotic causes of ACS

8
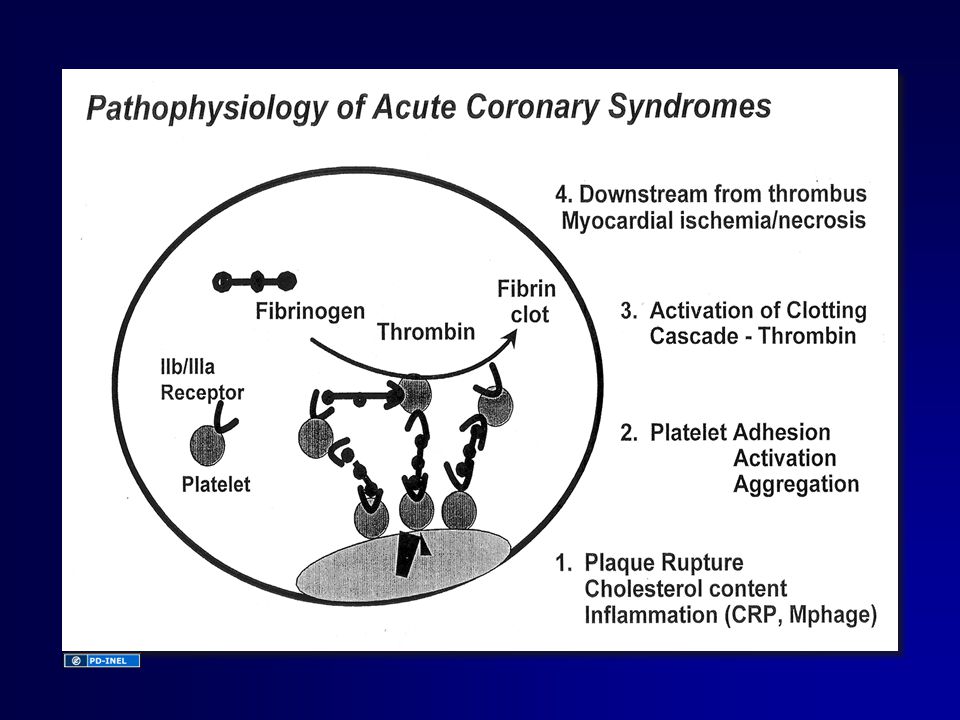
Pathogenesis: ACS > 90% - plaque disruption with platelet aggregation intracoronary thrombus Concepts of clot formation Continuum of ACS from unstable angina to STE MI

10
Acute Coronary Syndromes Unstable angina ST-Elevation MI (Q-wave MI) Non-ST Elevation MI (Non-Q-wave MI) Stable CAD The continuum of acute coronary syndromes ranges from unstable angina, through non-ST-elevation myocardial infarction (also referred to as “non-Q-wave” myocardial infarction [MI]), to ST-elevation MI (also referred to as “Q-wave” MI).
![Acute Coronary Syndromes Unstable angina ST-Elevation MI (Q-wave MI) Non-ST Elevation MI (Non-Q-wave MI) Stable CAD The continuum of acute coronary syndromes ranges from unstable angina, through non-ST-elevation myocardial infarction (also referred to as non-Q-wave myocardial infarction [MI]), to ST-elevation MI (also referred to as Q-wave MI).](http://images.slideplayer.com/19/5878390/slides/slide_10.jpg "Acute Coronary Syndromes Unstable angina ST-Elevation MI (Q-wave MI) Non-ST Elevation MI (Non-Q-wave MI) Stable CAD The continuum of acute coronary syndromes ranges from unstable angina, through non-ST-elevation myocardial infarction (also referred to as non-Q-wave myocardial infarction [MI]), to ST-elevation MI (also referred to as Q-wave MI).")
11
Normal Hemostasis 1st defense Platelets –“Primary hemostasis” Platelet plug 2nd defense Subendothelial –Tissue factor activates plasma –Coagulates proteins “Secondary hemostasis” Fibrin clot Vessel wall injury

12
Endogenous Antithrombotic Mechanisms Inactivation of clotting factors Antithrombin III Protein C / Protein S / thrombomodulin Tissue factor pathway inhibitor Lysis of fibrin clots Tissue plasminogen activator Endogenous platelet inhibition & vasodilation Prostacyclin Nitrous oxide

13
Endogenous Protective Mechanisms Lilly. Pathophysiology of Heart Disease, 4th Ed. Lippincott Williams, 2007. Page 170

14
Triggers to Plaque Rupture Inflammatory cytokines Plaque Rupture Physical Stress Vulnerable Plaque Emotional Stress

15
Mechanisms of Coronary Thrombosis Lilly. Pathophysiology of Heart Disease, 4th Ed. Lippincott Williams, 2007. Page 171

16
Consequences of Coronary Thrombosis Lilly. Pathophysiology of Heart Disease, 4th Ed. Lippincott Williams, 2007. Page 173

17
Causes of Acute Coronary Syndromes Atherosclerosis with superimposed thrombus Vasculitic syndromes Coronary emboli (e.g., from endocarditis, artificial valves) Congenital anomalies of the coronary arteries Coronary trauma or aneurysm Severe coronary artery spasm (primary or cocaine-induced) Increased blood viscosity (e.g., polycythemia vera, thrombocytosis) Significantly increased myocardial oxygen demand (e.g., aortic stenosis)
 Congenital anomalies of the coronary arteries Coronary trauma or aneurysm Severe coronary artery spasm (primary or cocaine-induced) Increased blood viscosity (e.g., polycythemia vera, thrombocytosis) Significantly increased myocardial oxygen demand (e.g., aortic stenosis)")
18
Extent of Myocardial Injury LV mass perfused by vessel Magnitude/Duration of flow Oxygen demand of affected tissue Adequacy of collaterals Tissue response to ischemia Determined by:

19
Acute Coronary Syndromes Unstable angina ST-Elevation MI (Q-wave MI) Non-ST Elevation MI (Non-Q-wave MI) Stable CAD The continuum of acute coronary syndromes ranges from unstable angina, through non-ST-elevation myocardial infarction (also referred to as “non-Q-wave” myocardial infarction [MI]), to ST-elevation MI (also referred to as “Q-wave” MI). Clinical Features: ACS
![Acute Coronary Syndromes Unstable angina ST-Elevation MI (Q-wave MI) Non-ST Elevation MI (Non-Q-wave MI) Stable CAD The continuum of acute coronary syndromes ranges from unstable angina, through non-ST-elevation myocardial infarction (also referred to as non-Q-wave myocardial infarction [MI]), to ST-elevation MI (also referred to as Q-wave MI).](http://images.slideplayer.com/19/5878390/slides/slide_19.jpg "Clinical Features: ACS.")
20
Unstable Angina Prior stable angina in: –Frequency –Duration –Intensity Angina at rest… previously only on provocation New onset angina

21
Acute Myocardial Infarction History and exam EKG changes Serum markers

22
Symptoms Pain Sympathetic response Parasympathetic response Inflammatory response Other –Pressure –Burning (hot) –Chest/arms/jaw/back –Sweats –Tachycardia –Cool, clammy skin –Nausea –Vomiting –Weak –Mild fever –Dyspnea –Asymptomatic
 –Chest/arms/jaw/back –Sweats –Tachycardia –Cool, clammy skin –Nausea –Vomiting –Weak –Mild fever –Dyspnea –Asymptomatic")
23
Physical Findings Inspection BP- often increase anterior MI - often decrease inferior MI HR- often increase anterior MI - often decrease inferior MI RA p o - increase in RV MI

24
Physical Findings Palpation LV Bulge- dyskinetic anterior wall Auscultation Gallop- S4-LV stiff Sounds- S3-LV fatigue Murmurs- Mitral regurgitation - VSD

25
Differential Diagnosis Cardiac Pericarditis - Sharp, pleuritic pain - PT prefers to sit - Friction rub - EKG diffuse STE Aortic Dissection - Instantaneous onset of severe pain - Pulse deficits or AI - Wide mediastinum (CXR)
")
26
Differential Diagnosis Pulmonary Pulmonary Embolus- Pleuritic pain - Dyspnea - Reason for clotting Pneumonia- Cough, sputum, fever - Consolidaton changes Gastrointestinal Esophageal Spasm- Retrosternal burning (acid) - After meals or at night
 - After meals or at night")
27
Diagnosis of ACS Typical symptomsCrescendo, rest, or new onset severe angina Serum biomarkersNoYesYes ECG initial findingsST depression and/or ST depression and/ST elevation (and Q T wave inversionor T wave inversionwaves later) Unstable AnginaMyocardial Infarction Prolonged “crushing” chest pain, more severe and wider radiation than usual angina NSTEMISTEMI NSTEMI, non-ST-elevation myocardial infarction (MI); STEMI, ST-elevation MI
 Unstable AnginaMyocardial Infarction Prolonged crushing chest pain, more severe and wider radiation than usual angina NSTEMISTEMI NSTEMI, non-ST-elevation myocardial infarction (MI); STEMI, ST-elevation MI")
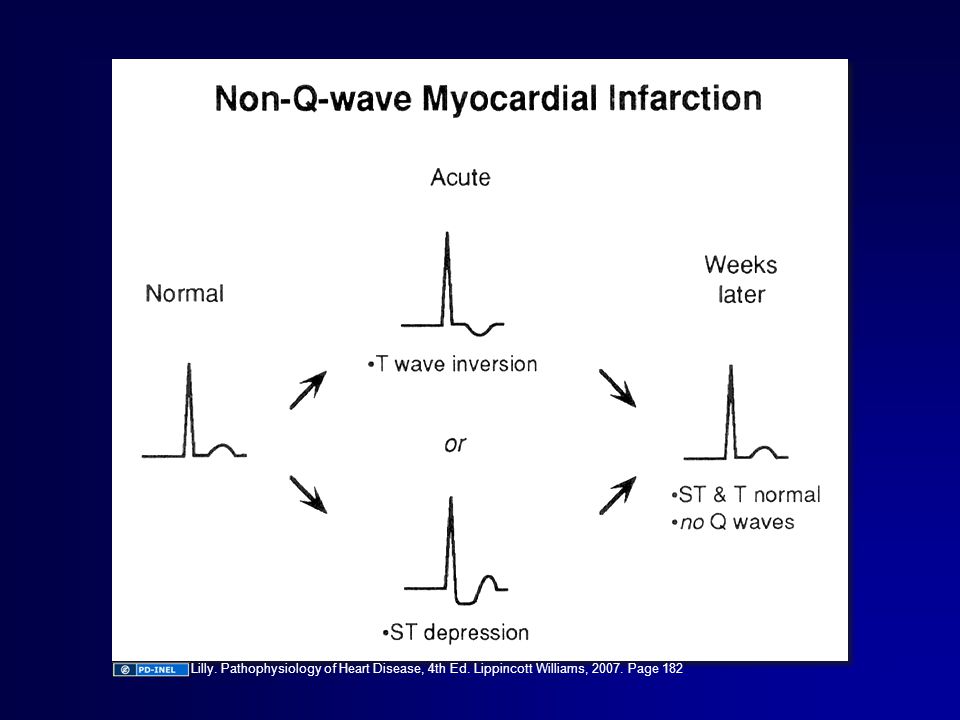
28
Lilly. Pathophysiology of Heart Disease, 4th Ed. Lippincott Williams, 2007. Page 182

30
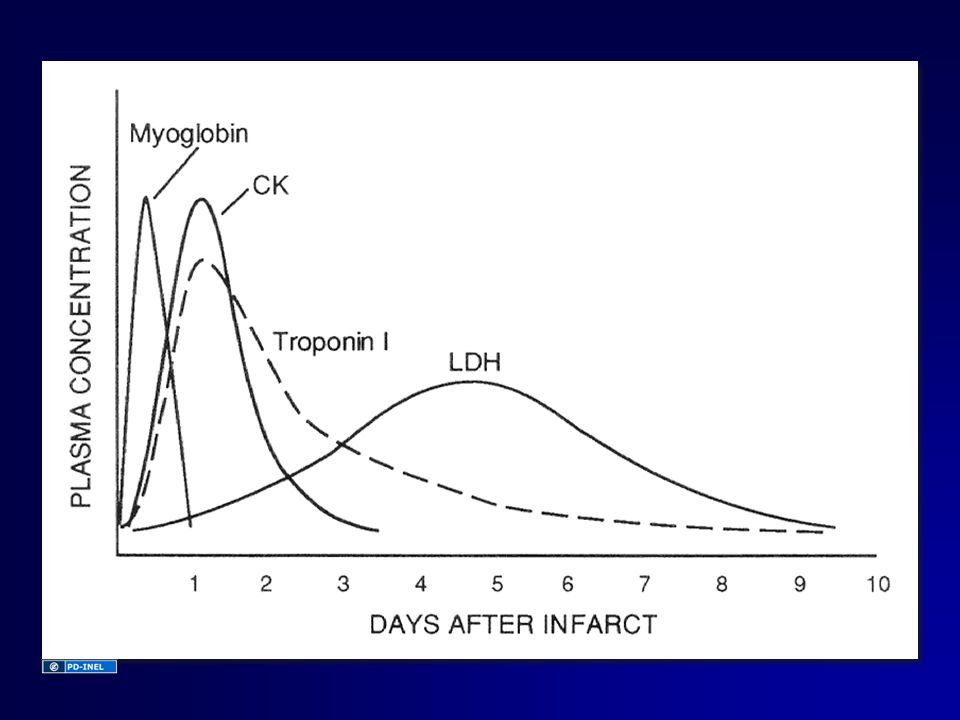
Serum Markers of Myocardial Infarction Myocardial necrosis causes sarcolemma disruption Intracellular macromolecules are released Can be measured by serial blood testing Pattern and level of rise correlates with timing and size of MI

31
Cardiac-Specific Troponins Regulatory protein that controls interaction between actin & myosin 3 subunits: TnC, I, T Unique cardiac troponins I and T exist - absent in serum of healthy people Powerful marker of myocyte damage Rise at 3-4 hours post-MI, peak 18-36 hrs, decline slowly 10-14 days Skeletal & cardiac muscle

32
Creatinine Kinase Enzyme that converts ADP to ATP Found in many tissues: heart, brain, skeletal muscle, kidney, etc. Can be elevated after injury to any of these tissues 3 isoenzymes:- CK-MM - CK-MB - CK-BB

33
CPK-MB Makes up 1-3% of skeletal CK Makes up much higher % of cardiac CK Rises 4-8 hours after MI, peaks by 24 hours Returns to normal in 48-72 hours

35
Treatment of Acute Coronary Syndromes: STE vs. Non STE

36
Treatment of Acute Coronary Syndromes Anti-ischemic therapiesAnti-ischemic therapies General measures:General measures: Antithrombotic therapiesAntithrombotic therapies Antiplatelet agents: Anticoagulants (use one): Adjunctive therapies:Adjunctive therapies: Β-blockerΒ-blocker NitratesNitrates +/- Calcium channel blocker+/- Calcium channel blocker Pain control (morphine)Pain control (morphine) Supplemental O 2 if neededSupplemental O 2 if needed AspirinAspirin Clopidogrel (or prasugrel)Clopidogrel (or prasugrel) GP IIb/IIIa inhibitor (for selected high risk patients; may be deferred until PCI)GP IIb/IIIa inhibitor (for selected high risk patients; may be deferred until PCI) LMWH (enoxaparin)LMWH (enoxaparin) Unfractionated intravenous heparinUnfractionated intravenous heparin FondaparinuxFondaparinux Bivalirudin (should be used in ACS patient only if undergoing PCI)Bivalirudin (should be used in ACS patient only if undergoing PCI) StatinStatin Angiotensin converting-enzyme inhibitorAngiotensin converting-enzyme inhibitor
: Adjunctive therapies:Adjunctive therapies: Β-blockerΒ-blocker NitratesNitrates +/- Calcium channel blocker+/- Calcium channel blocker Pain control (morphine)Pain control (morphine) Supplemental O 2 if neededSupplemental O 2 if needed AspirinAspirin Clopidogrel (or prasugrel)Clopidogrel (or prasugrel) GP IIb/IIIa inhibitor (for selected high risk patients; may be deferred until PCI)GP IIb/IIIa inhibitor (for selected high risk patients; may be deferred until PCI) LMWH (enoxaparin)LMWH (enoxaparin) Unfractionated intravenous heparinUnfractionated intravenous heparin FondaparinuxFondaparinux Bivalirudin (should be used in ACS patient only if undergoing PCI)Bivalirudin (should be used in ACS patient only if undergoing PCI) StatinStatin Angiotensin converting-enzyme inhibitorAngiotensin converting-enzyme inhibitor")
37
Treatment of Acute Coronary Syndromes ST-Elevation (STEMI) Emergent PCI available within 90 min? Fibrinolytic Therapy (e.g., tPA) Non-ST-Elevation (UA and NSTEMI) Risk Assessment (e.g., GRACE Score) Primary PCIConservative Strategy (Proceed to cardiac cath only if recurrent angina or predischarge stress test is markedly positive) Invasive Strategy (Cardiac cath leading to PCI or CABG) NoYesLowHigh
 Non-ST-Elevation (UA and NSTEMI) Risk Assessment (e.g., GRACE Score) Primary PCIConservative Strategy (Proceed to cardiac cath only if recurrent angina or predischarge stress test is markedly positive) Invasive Strategy (Cardiac cath leading to PCI or CABG) NoYesLowHigh.")
38
I

39
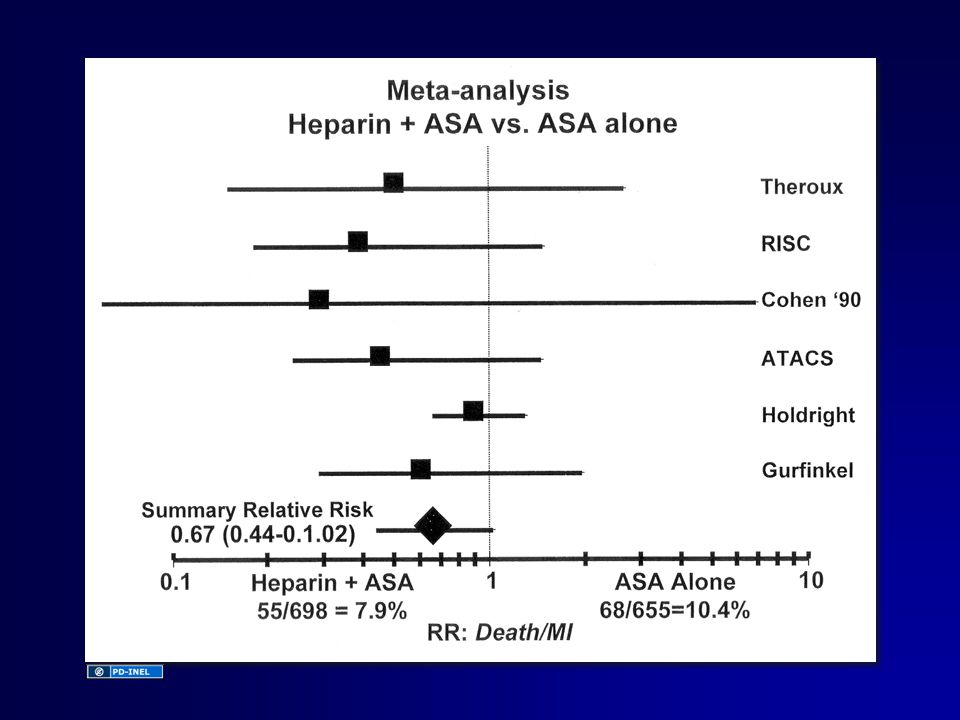
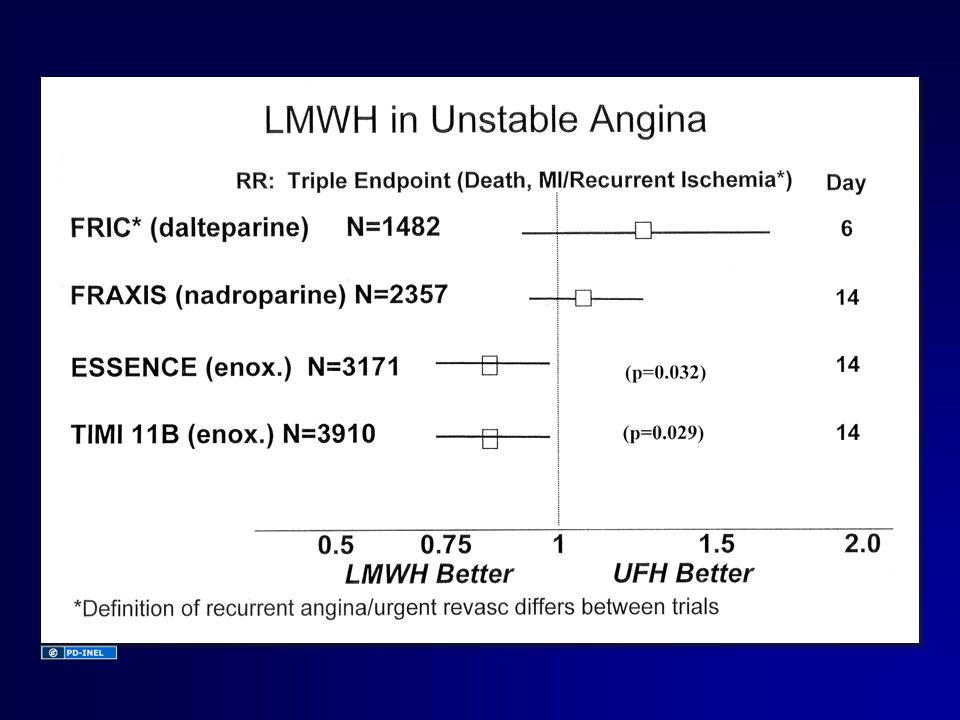
Antithrombin Rx Factor X TF / VII a Factor X a LMWH V Ca ++ UFH ProthrombinThrombin Hirudin Fibrinogen Fibrin Clot

43
Nitrates Reduce ischemia (not mortality) Venodilation: R heart return Coronary vasodilation Usually given SL then IV
 Venodilation: R heart return Coronary vasodilation Usually given SL then IV")
44
Beta Blockers Sympathetic drive; HR & BP O 2 demand Shear stress Sudden death, death, recurrent MI

45
Non Dihydropyridine Calcium Channel Blockers Heart rate Vasodilate Relieve ischemia, not mortality Don’t give in patients with sx/signs of heart failure

46
Non - STE ACS: Conservative vs. Early Invasive Approach

47
Early Invasive Urgent catheterization performed after initial medical Rx Allows rapid identification & Rx of critical CAD More PCI/CABG

48
Conservative Cath patients with recurrent ischemia in hospital Cath patients with inducible ischemia on pre-discharge stress test

49
Invasive vs. Conservative Recent clinical trials show less infarction/reinfarction & possibly death with invasive strategy Especially in higher risk patients: –ST segment deviation –Elevated biomarkers –Multiple risk factors… esp. DM

50
Acute Treatment: STE MI Reperfusion: Thrombolysis vs. PTCA ASA O 2 Beta blockers Nitrates ACE inhibitors Morphine Anticoagulants

51
A A Lilly. Pathophysiology of Heart Disease, 4th Ed. Lippincott Williams, 2007. Page 188

52
B B

53
PCI vs. Lytic Short-Term Outcomes Frequency (%) Long-Term Outcomes P=0.0002 P=0.0003 P<0.0001 P<0.0001 P=0.0004 P<0.0001 P<0.032 P<0.0001 P=0.0019 P=0.0053 P<0.0001 P<0.0001 P<0.0001DeathDeathExcludingSHOCKNonfatalMIRecurrentIschemiaTotalCVAIntra-CranialBleedMajorBleedDeath/CVA/MI Circ 2003; 107: 2538-2542
 Long-Term Outcomes P= P= P< P< P= P< P<0.032 P< P= P= P< P< P<0.0001DeathDeathExcludingSHOCKNonfatalMIRecurrentIschemiaTotalCVAIntra-CranialBleedMajorBleedDeath/CVA/MI Circ 2003; 107:")
54
Additional Rx: STE MI Maintain vessel patency Restore balance between 0 2 supply and demand Relieve chest pain Prevent complications

55
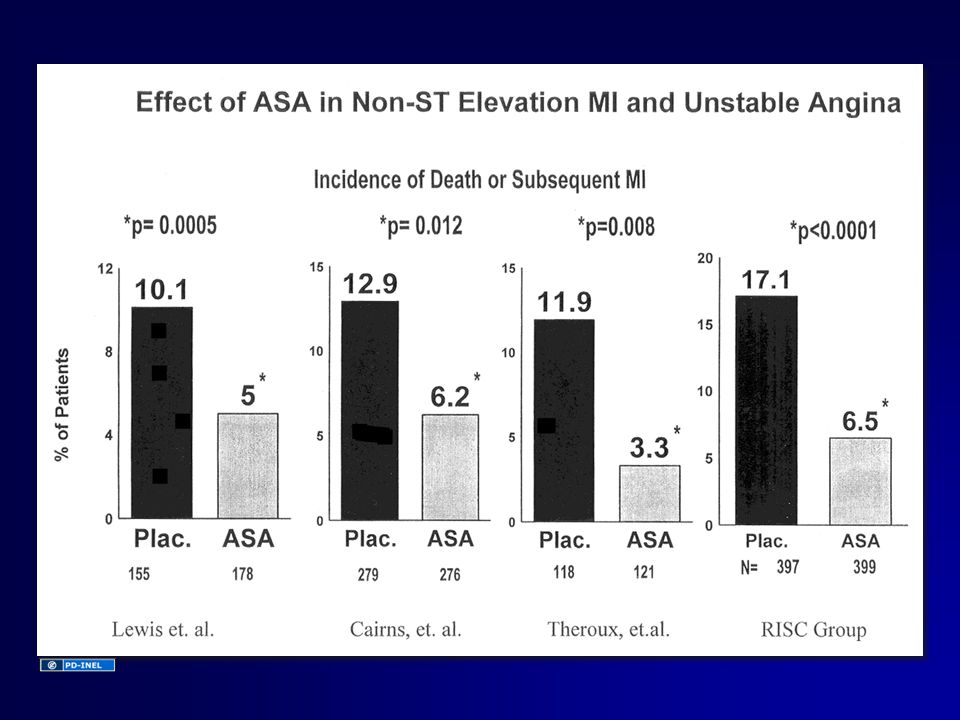
Aspirin Reduces mortality & reinfarction Give immediately on presentation and daily thereafter If aspirin allergy, use clopidogrel

56
Heparin Give 1-2 days IV after PCI or lysis with tPA, rPA, or TNK-tPA… NOT SK Also if: –Atrial fibrillation –LV thrombus –New anterior MI with large wall motion change All others: SQ heparin while at bed rest to prevent DVT

57
ß- Blockers Risk arrhythmia, reinfarction, rupture, death Give IV, then orally unless contraindication exists (asthma, hypotension, significant bradycardia)
")
58
Nitrates Reduce pain/ischemia Relieve pain Reduce pulmonary congestion in heart failure

59
ACE - Inhibitors Limit adverse LV remodeling Heart failure/death MI Benefit additive ASA, BB Esp. benefit anterior MI and/or LV dysfunction

60
Statins Reduce reinfarction, death More benefit when started early Give if LDL cholesterol is > 100

61
Acute MI: Complications Recurrent ischemic/reinfarction Arrhythmias Myocardial dysfunction Mechanical complications Pericarditis Thromboembolism

62
Complications of MI Myocardial Infarction Ventricularthrombus Contractility Contractility ElectricalinstabilityTissuenecrosisPericardialinflammation EmbolismArrhythmiasPericarditis Papillarymuscleinfarction/ischemiaVentricularseptaldefectVentricularrupture Mitralregurgitation Congestive heart failure Coronary Coronaryperfusionpressure Ischemia IschemiaHypotension Cardiogenicshock Cardiactamponade

63
Recurrent Ischemia Angina or ischemia confers increase risk for reinfarction Should lead to angiography and revascularization for most pts.

64
Arrhythmias in Acute MI Sinus Bradycardia - Vagal tone - SA nodal artery perfusion Sinus Tachycardia - CHF - Volume depletion - Pericarditis - Chronotrophic drugs (e.g. Dopamine) APB’s, atrial fib, - CHF VPB’s, VT, VF - Atrial Ischemia - Ventricular ischemia - CHF AV block (1 o, 2 o, 3 o ) - IMI: Vagal tone and AV nodal artery flow - AMI: Extensive destruction of conduction tissue RhythmCause
 APB’s, atrial fib, - CHF VPB’s, VT, VF - Atrial Ischemia - Ventricular ischemia - CHF AV block (1 o, 2 o, 3 o ) - IMI: Vagal tone and AV nodal artery flow - AMI: Extensive destruction of conduction tissue RhythmCause.")
65
Blood Supply in the Conduction System SA node- RCA (70% of patients) AV node- RCA (85% of patients) Bundle of His- LAD (septal branches) RBB- Proximal portion by LAD - Distal portion by RCA LBB Left anterior fascicle- LAD Left posterior fascicle- LAD and PDA C onduction P athway P rimary A rterial S upply
 AV node- RCA (85% of patients) Bundle of His- LAD (septal branches) RBB- Proximal portion by LAD - Distal portion by RCA LBB Left anterior fascicle- LAD Left posterior fascicle- LAD and PDA C onduction P athway P rimary A rterial S upply")
66
Myocardial Dysfunction Congestive Heart Failure –Systolic or diastolic –Treated with vasodilators, diuretics, and Rx to reverse ischemia Cardiogenic Shock –Depressed CO –Hypotension –Poor perfusion of vital organs –Treatment: Look/Treat reversible cause –Inotropes/vasodilators/IABP

67
Cardiogenic Shock - MI - 1Y Initial Medical Stabilization - n=150 Time From Randomization, mo Proportion Alive 0 Early Revascularization - n=152 Shock (JS Hochman et al.) JAMA 2001; 285:190 1.0 0.8 0.6 0.4 0.2 0 24681012 Benefit < 75 Years
 JAMA 2001; 285: Benefit < 75 Years")
68
RV Infarction Common in IMI’s Sx/signs: –Hypotension –Increase RA Pressure Rx: –Volume, hemodynamic monitoring…PA line

69
Papillary Muscle Infarction “Common” in inferoposterior MI Leads to acute mitral valve regurgitation Left heart failure/pulmonary edema Rx: Coronary revascularization; IABP; valve repair

70
Free Wall Rupture More likely in elderly, HTN, women Usually rapidly fatal Occasional walls off to form pseudoaneurysm Urgent surgery is best chance

71
Ventricular Septal Defect Heralded by left to right shunting at ventricular level RV volume overload Loud systolic murmur over sternum Usually requires surgical repair

72
True Ventricular Aneurysm Occurs late More often in non-reperfused STE MI’s Complications: Clot, CHF, arrhythmias

73
Pericarditis More common in non-reperfused STE MI Fever, sharp pain with pleuritic tendency, friction rub Treatment: nonsteroidal anti-inflammatory agent; heparin relatively contraindicated

74
Thromboembolism Clot forms on infarcted akinetic myocardium Most common in large anterior MI Can cause embolic stroke Rx: 3-6 months anticoagulants If clot seen on echo or LVEF < 30% or if large anterior MI

75
Predictor of Poor OutcomeMethod to DetectTreatment Poor LVEFEchocardiogramACE, BB Residual IschemiaPre D/C ETTCath; ASA,BB Max ETT later ArrhythmiasMonitoring/Directed Observation Post MI Risk Stratification and Management

76
Standard Discharge Rx 3 to 5 day length of stay ASA; clopidogrel Beta blocker ACE for CHF; LVEF < 40%, perhaps all Warfarin as noted Cardiac Rehab PRN Nitrates Exercise prescription Low fat diet Smoking Cessation Statin if LDL cholesterol > 100 mg/dl

77
Kaplan–Meier Cumulative Risk of the Primary Outcome, Stratified According to GRACE Risk Score at Baseline Mehta SR NEJM 2009;360:2172 Mehta SR et al. NEJM 2009;360:2172.

Similar presentations

: Prachi Agarwal M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution–Non-commercial–Share.>")
: Caroline Richardson, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution–Noncommercial–Share.>")

: John Doe, MD; Jane Doe, PhD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution.>")


: Louis D’Alecy, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution–Non-commercial–Share.>")


 CAD is most common form of heart disease and causes premature death. In UK, 1 in 3 men and.>")


. ACS Pathophysiology is that of a ruptured or eroded atheromatous plaque. Pathophysiology is that of a ruptured or eroded.>")
: Peter Moyer (Boston University), MD, MPH 2012 License: Unless otherwise.>")




