Caudal Anaesthesia

Take home messages
- One of the most commonly examined regional blocks in children, generally for surgery below the umbilicus
- Also used in chronic pain management in adults
- You need to know the Armitage regimen, and why it's risky
If you just want the OSCE answer on how to perform it
Generally for the exam they want you to describe the landmark technique, rather than the fluoroscopically guided or ultrasound guided methods.
Preparation (as always)
- Consent and identity check
- Monitoring and skilled assistance
- Emergency drugs and equipment
- IV access, and if paediatric patient, probably already under general anaesthesia
- Position appropriately - prone or lateral with legs curled up to chest
- Full sterile precautions
Find the sacral hiatus
- Palpate the posterior superior iliac spines
- Imagine an equilateral triangle between these PSIS and the coccyx
- The sacrial hiatus is at the apex of this triangle, just inferomedial to the sacral cornua
- Insert 22g cannula at 45° (pointing towards the patient's xiphisternum)
- There should be a 'click' as it punctures the sacrococcygeal ligament
- Then lower the needle to be parallel to the sacral canal and advance a few mm further
- Remove the needle and leave the cannula in place
Injection
- Aspirate the cannula first, to rule out intrathecal or intravascular injection
- Draw up your local anaesthetic*
- Inject slowly
*Drawing your drugs up leaving the cannula in place after aspirating allows a little more time for any CSF or blood to make itself known - a negative initial aspiration doesn't completely rule out incorrect placement, and sometimes this technique will save you a lot of stress
If you just want a video
This is our absolute favourite video from the amazing @regionalanaesthesiology who you should go and subscribe to right now.
A spot of history
So the Latin word 'sacrum' means sacred.
I didn't personally consider the sacrum to be all that sacred when trying to learn its anatomy, but apparently it was an important animal bone for a variety of rituals throughout history.
(Or they mistranslated from the Greek word for 'strong', which is less interesting but more logical.)
In 1901 two Frenchmen by the names of Cathelin and Sicard described the concept of injecting local anaesthetic into the caudal space, twenty years before anyone thought to stick a needle in the lumbar epidural space.
The problem was that it had rather a high failure rate at the time, what with people's variable anatomy and the lack of ultrasound, so it was shelved for many years until a resurgence of interest during the 1940s.
It has since been widely used - particularly in paediatric surgery - for both analgesia and anaesthesia and continues to be employed in many hospitals, however this review article suggests we're probably headed towards other more reliable blocks what with the advent of ultrasound and all that.
But it will remain FRCA-examinable forever.
When can it be used?
Any time you want to provide analgesia or anaesthesia to the lower half of a human body, you can consider doing a caudal block.
We do them a lot more in kids, because the caudal space is a lot easier to find in kids than in adults, and generally simpler to perform than a lumbar epidural or alternative technique.
It also tends to have fewer side effects and lower risk of complications than aiming a needle at an infant's spinal canal.
What are the indications for caudal anaesthesia?
- Surgical anaesthesia and postoperative analgesia
- Acute low back or pelvic pain
- Acute and chronic lumbar radiculopathy
- Diabetic neuropathy
- Herpes Zoster pain and post herpetic neuralgia
- Hidradenitis suppurativa
- Cancer pain
Why would I choose caudal over lumbar epidural?
- Faster onset of saddle block (perineal anaesthesia)
- Better sacral coverage for foot surgery
- Previous spinal surgery or lumbar deformity contraindicating lumbar epidural
- Vastly lower risk of inadvertent dural puncture and post dural puncture headache
Why does age matter?
This procedure can be performed in pretty much any aged patient, but it's important to understand the anatomical differences that occur around puberty.
Also, in around 8% of children, the dural sac can still terminate below S2.
What anaesthetic agent should you use for a paediatric caudal block and what dose?
0.25% Bupivacaine or levobupivacaine, or ropivacaine 0.2% are recommended.
For the exam you need to know the Armitage regimen:
- 0.5ml/kg for a sacro-lumbar block
- 1ml/kg for mid-abdominal block
- 1.2ml/kg for mid-thoracic block
However this isn't actually very good at predicting the height of the block, and weirdly 1.2ml/kg of 0.25% bupivacaine is by definition above the recommended safe dose of 2mg/kg.
Adults have much denser epidural fat, meaning the drug doesn't spread towards the head nearly as reliably as in children.
Who can't have it?
Ah yes, the classic OSCE and CRQ question on 'contraindications to regional anaesthesia'.
You can score at least four marks without knowing anything at all about the procedure itself, because the contraindications to any regional procedure are:
- Patient or guardian refusal
- Local infection over site of needle injection
- Allergy to local anaesthetic
- Severe coagulopathy
Meanwhile the contraindications specific to caudal anaesthesia are:
- Raised intracranial pressure
- Significant anatomical abnormality such as tethered cord syndrome
- Pilonidal cyst
What are the risks?
- Block failure
- Damage to surrounding structures, including blood vessels, nerve roots and bowel
- Accidental intravascular subdural or intrathecal injection
- Infection - meningitis, epidural abscess
- Hypotension
- Bleeding - epidural haematoma
- Local anaesthetic systemic toxicity - more common after caudal than other blocks
Podcast Episode
Useful Tweets
Ultrasound-guided sacral multifidus plane block for analgesia following excision of sacrococcygeal teratoma in two neonates
— 𝘈𝘯𝘢𝘦𝘴𝘵𝘩𝘦𝘴𝘪𝘢 𝘙𝘦𝘱𝘰𝘳𝘵𝘴 (@Anaes_Reports) April 27, 2021
This block may be a viable alternative to caudal anaesthesia for peri-operative analgesia.
🔗https://t.co/KYd0JVz4Hk#freetoread #regionalanaesthesia pic.twitter.com/3EKja6ptuw
🔐This new report from @anesthetix describes how the routine use of ultrasound for caudal anaesthesia resulted in the identification of perineural cysts and a subsequent change in analgesic management.#FreeForAWeek #PaedsAnaes
— 𝘈𝘯𝘢𝘦𝘴𝘵𝘩𝘦𝘴𝘪𝘢 𝘙𝘦𝘱𝘰𝘳𝘵𝘴 (@Anaes_Reports) November 18, 2020
🔗https://t.co/9V1RfF2Wp7 pic.twitter.com/Js9xsGS65g
CSF Tap during caudal #AORA23- since there was no literature as to what to do, I polled the members and executive committee of the Indian association of pediatric anaesthesia - and this is what the experts had to say - @AoraIndia @ESRA_trainees @ESRA_Society @ASRA_Society pic.twitter.com/iKN1zcktWL
— Vedhika shanker (@vedhika_shanker) June 5, 2023
References and Further Reading
 NYSORA
NYSORA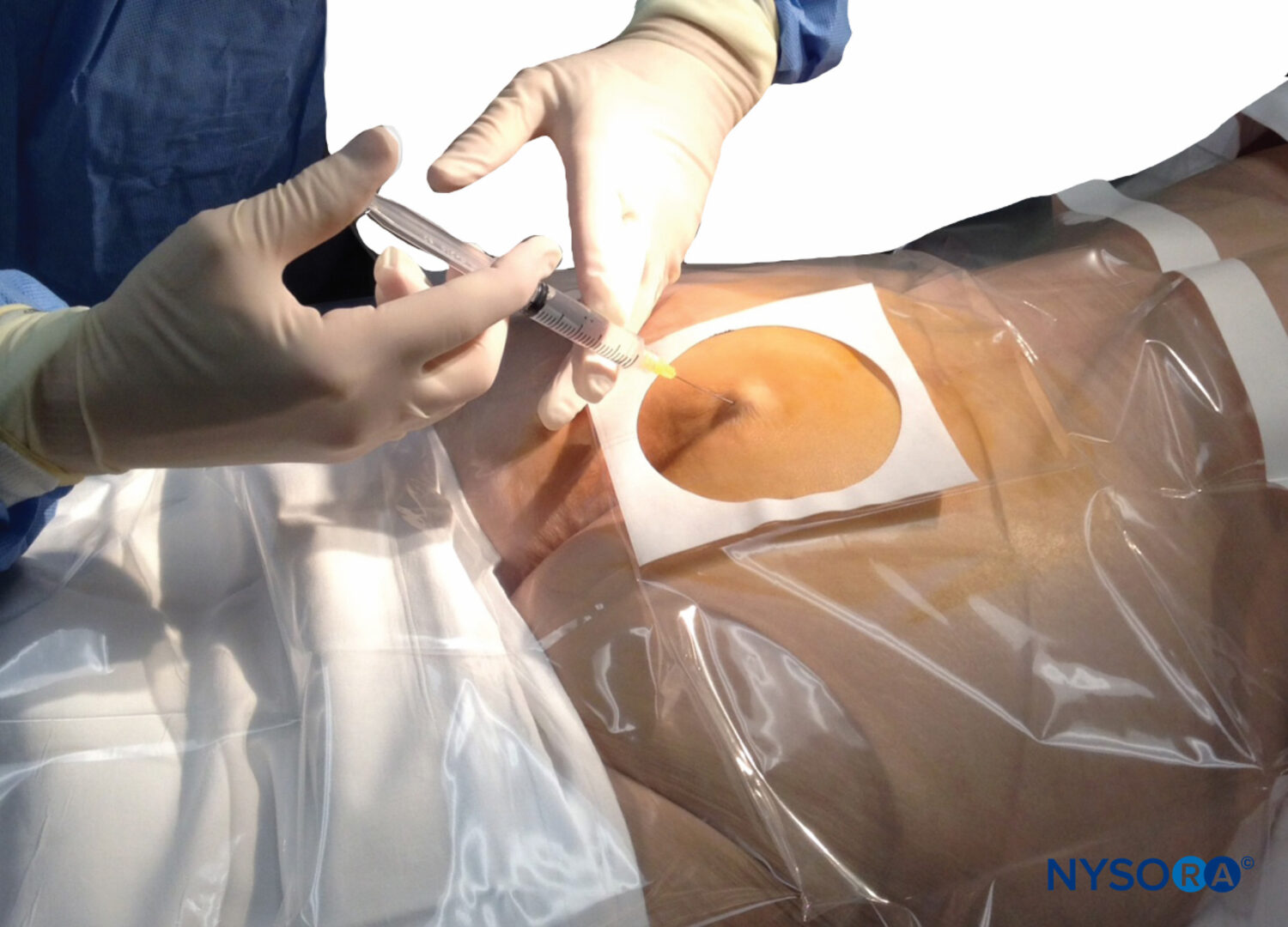
Primary FRCA Toolkit
Members receive 60% discount off the FRCA Primary Toolkit. If you have previously purchased a toolkit at full price, please email anaestheasier@gmail.com for a retrospective discount.

Discount is applied as 6 months free membership - please don't hesitate to email Anaestheasier@gmail.com if you have any questions!
Just a quick reminder that all information posted on Anaestheasier.com is for educational purposes only, and it does not constitute medical or clinical advice.