ANTI-ANGINAL THERAPY
Anti-anginal Therapy
Basic Facts
- Angina pectoris results from a condition called coronary heart disease, an accumulation of plaque inside the coronary blood vessels that reduces blood flow to the heart.
- The pain or tightness associated with angina results from ischemia, the lack of oxygen-carrying blood reaching the heart.
- The goals of drug therapy for angina are to relieve ischemia, reduce the frequency and severity of angina attacks, and prevent heart attack.
- Medications that control angina symptoms and ischemia include nitrates, beta-blockers, and calcium channel blockers. To treat the underlying coronary heart disease, physicians use antiplatelets, lipid-lowering agents, and drugs to control high blood pressure and diabetes.
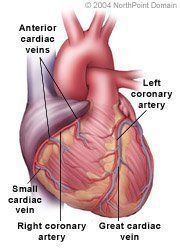
Angina pectoris is chest pain or discomfort. A person may feel pain when insufficient oxygen-rich blood reaches the heart muscle. This reduced blood flow is caused by coronary heart disease (CHD), an accumulation of plaque inside the coronary blood vessels.
Angina that occurs unpredictably or during rest is called unstable angina. Sometimes, unstable angina can result from a temporary blood clot that suddenly blocks blood flow to the heart. The pain subsides when the clot dissolves and blood flow resumes.
If a person has experienced angina after exertion, called stable angina, and angina symptoms begin to last after exercise or occur at rest, the angina may have become unstable angina. This usually means an artery has narrowed further, often because of a blood clot. If an episode of unstable angina is the first instance of angina a person experiences, it is called new onset unstable angina.
The goals of angina medication and treatment are to relieve ischemia, thereby reducing the frequency and severity of angina attacks and preventing a heart attack. It is important to know in advance the various side effects of any medication and to be aware of serious side effects that may require medical attention. Some medications can interact with substances in a way that can alter the effect the medication has on the body, so people with angina should tell their physician about other prescriptions, their alcohol consumption, or any herbal supplements they take.
WHAT TO EXPECT
Medications that control angina symptoms and ischemia include nitrates, beta-blockers, and calcium-channel blockers.
Nitrates. Nitrates, or nitroglycerin, are the most commonly prescribed drugs for angina. Nitrates are vasodilator drugs, meaning that they widen blood vessels, allowing more blood to flow to the heart through the coronary arteries and relieving pain.
Some nitrates take effect in as little as 2 minutes and are taken when discomfort occurs or is expected, such as for stable angina that occurs during exertion or stress. These short-acting nitrates may come in the form of a liquid that is sprayed into the mouth or a tablet that is placed under the tongue. Longer-acting nitrates that may be taken before unstable angina symptoms occur come in pill, ointment, or patch form. Depending on the formulation, the effects of nitrates last from 30 minutes to 24 hours. Nitrates may cause side effects including:
- Dizziness;
- Lightheadedness; or
- Headaches.
One drawback to the use of nitrates is that people can develop a tolerance to them, limiting their effectiveness over time.
Beta-Blockers slow the heart rate by blocking the effect that adrenaline has on the heart. Limiting the heart rate during exercise and reducing the heart's oxygen needs can delay the onset of an angina attack in people with stable angina. Long-acting beta-blockers reduce symptoms in people who have unstable angina.
Side effects of beta-blockers include:
- Depression;
- Dizziness;
- Weakness;
- Fatigue;
- Lightheadedness;
- Sexual dysfunction; and
- Sleep disturbances.
Depending on the dose, beta-blockers usually take effect in 15 minutes to 1 hour and act from12 hours to 24 hours.
Calcium-channel blockers cause coronary blood vessels to dilate and blood pressure to drop, increasing blood flow through the heart and reducing angina symptoms. Like nitrates, calcium-channel blockers are effective in reducing the frequency and severity of angina attacks by decreasing the resistance the heart faces when pumping blood, thereby lessening the heart's demand for oxygen.
Side effects of calcium-channel blockers include:
- Constipation;
- Dizziness;
- Nausea;
- Low blood pressure; and
- Headache.
The other goal of angina therapy, preventing a heart attack, is accomplished by controlling the underlying CHD that causes angina. Doctors use anti-platelets, lipid-lowering agents, and anticoagulants to prevent CHD from contributing to a heart attack.
Anti-platelet medications, such as aspirin, may be prescribed to people with stable and unstable angina. Though aspirin is the most commonly prescribed anti-platelet, other anti-platelets available to people who are allergic to aspirin include the fast-acting clopidogrel and, less commonly, the slower-acting ticlopidine. In addition, these drugs may be prescribed alone or in conjunction with aspirin.
Lipid-lowering agents. Common lipid therapy medications prescribed to people with stable and unstable angina in an effort to slow the progression of CHD and prevent a heart attack include:
- Statins;
- Bile acid sequestrants;
- Fibrates; and
- Niacin (Vitamin B5).
Anticoagulant drugs that prevent blood from clotting are used to prevent heart attacks in people who go to the hospital with an attack of unstable angina. Heparin is an anticoagulant that inhibits reactions that lead to the clotting of blood and the formation of fibrin, a protein in blood that is essential to the formation of a blood clot. To prevent a heart attack, heparin may be given intravenously for up to 48 hours after an attack of unstable angina. Another anticoagulant, warfarin, which acts against different blood clotting factors and proteins, may be prescribed to people with unstable angina for a period of months to decrease the risk of blood clots causing repeat angina attacks or a heart attack.
Doctors recommend that people who have stable or unstable angina make certain lifestyle changes aimed at reducing high blood pressure and high cholesterol levels, including:
- Smoking;
- Diet; and
- Exercise.
When a person's angina does not respond to medication and lifestyle changes, and a person remains at risk of a heart attack, doctors may recommend one of the following treatments:
- Angioplasty. A balloon-carrying catheter is inserted into a blood vessel in the arm or groin and is guided through blood vessels and into a blocked coronary artery. The physician inflates the balloon and the pressure from the balloon flattens the plaque against the artery wall, increasing the artery's diameter. In most cases, a stent, a metal-mesh tube, is expanded under the plaque and left inside the artery to serve as scaffolding that keeps the artery widely open.
- Bypass surgery. In this procedure, known as coronary artery bypass graft, or CABG, a physician uses new blood vessels taken from a person's leg or chest to bypass, or reroute blood around, any blockages in one or more arteries in the heart.
Copyright © 2017 NorthPoint Domain, Inc. All rights reserved.
This material cannot be reproduced in digital or printed form without the express consent of NorthPoint Domain, Inc. Unauthorized copying or distribution of NorthPoint Domain's Content is an infringement of the copyright holder's rights.