
An Unconventional Oral Candidiasis in an Immunocompetent Patient
 , , ,
, , ,  , , and
, , and
Abstract
:1. Introduction
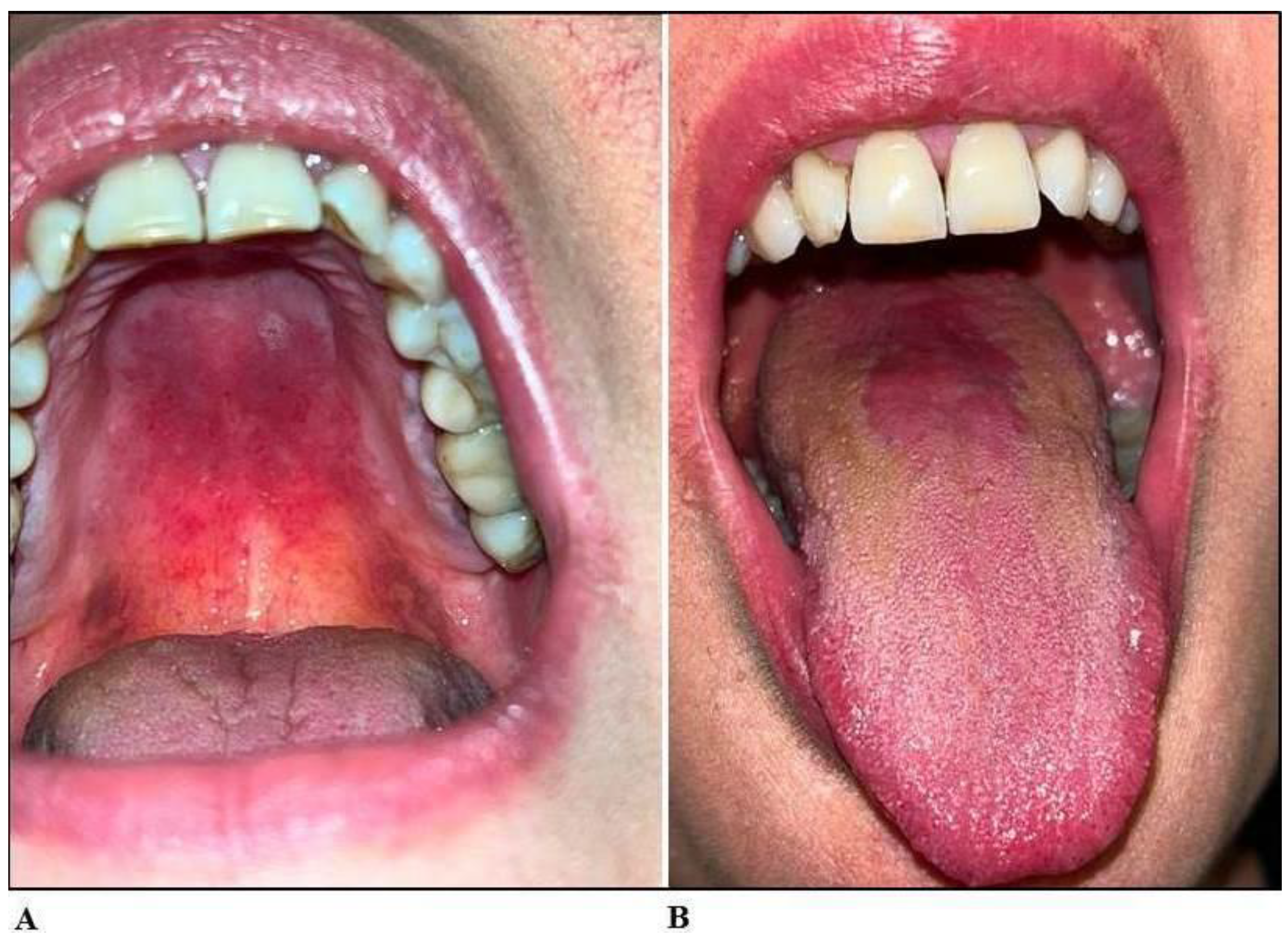
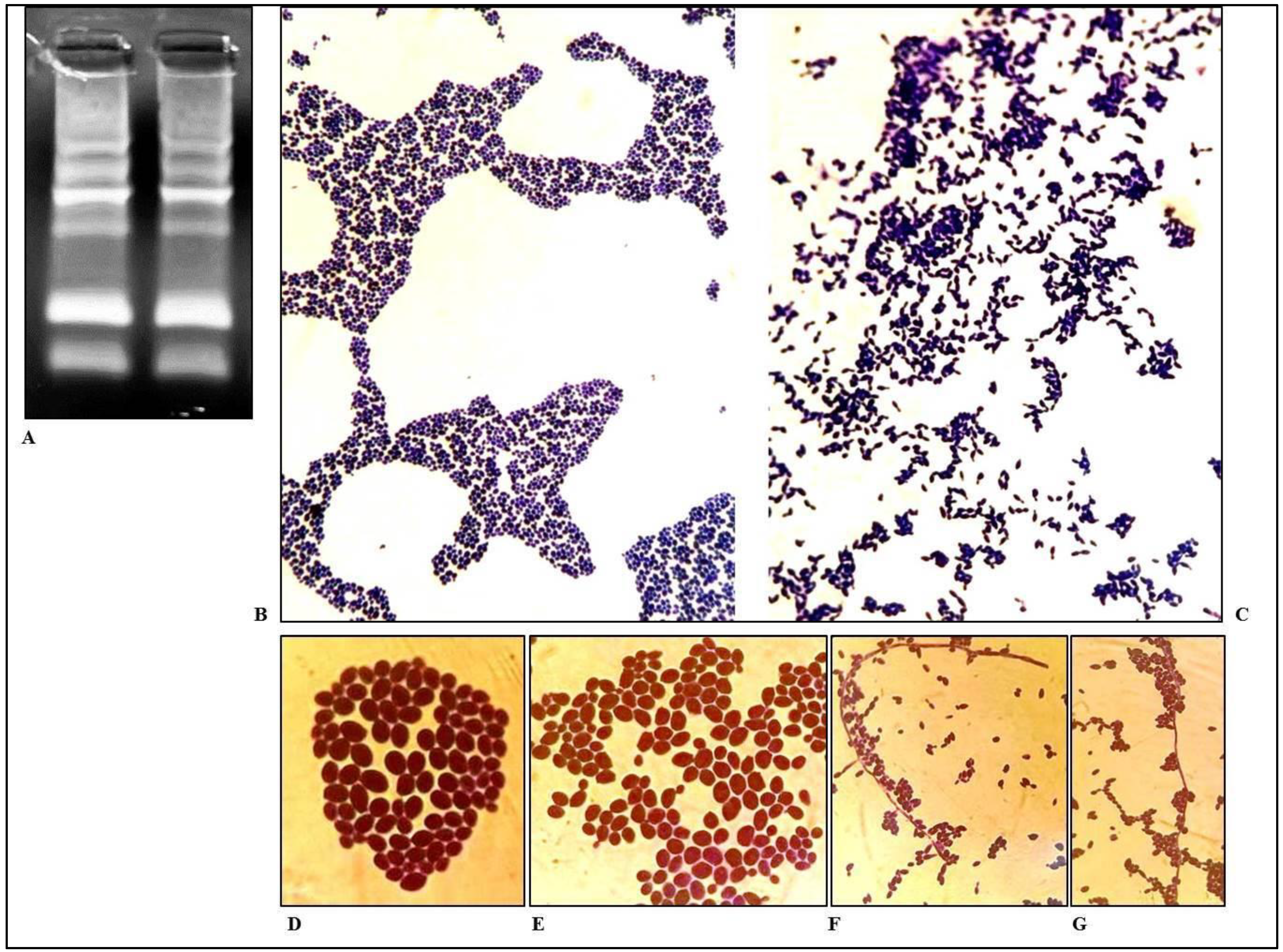
2. Case Report
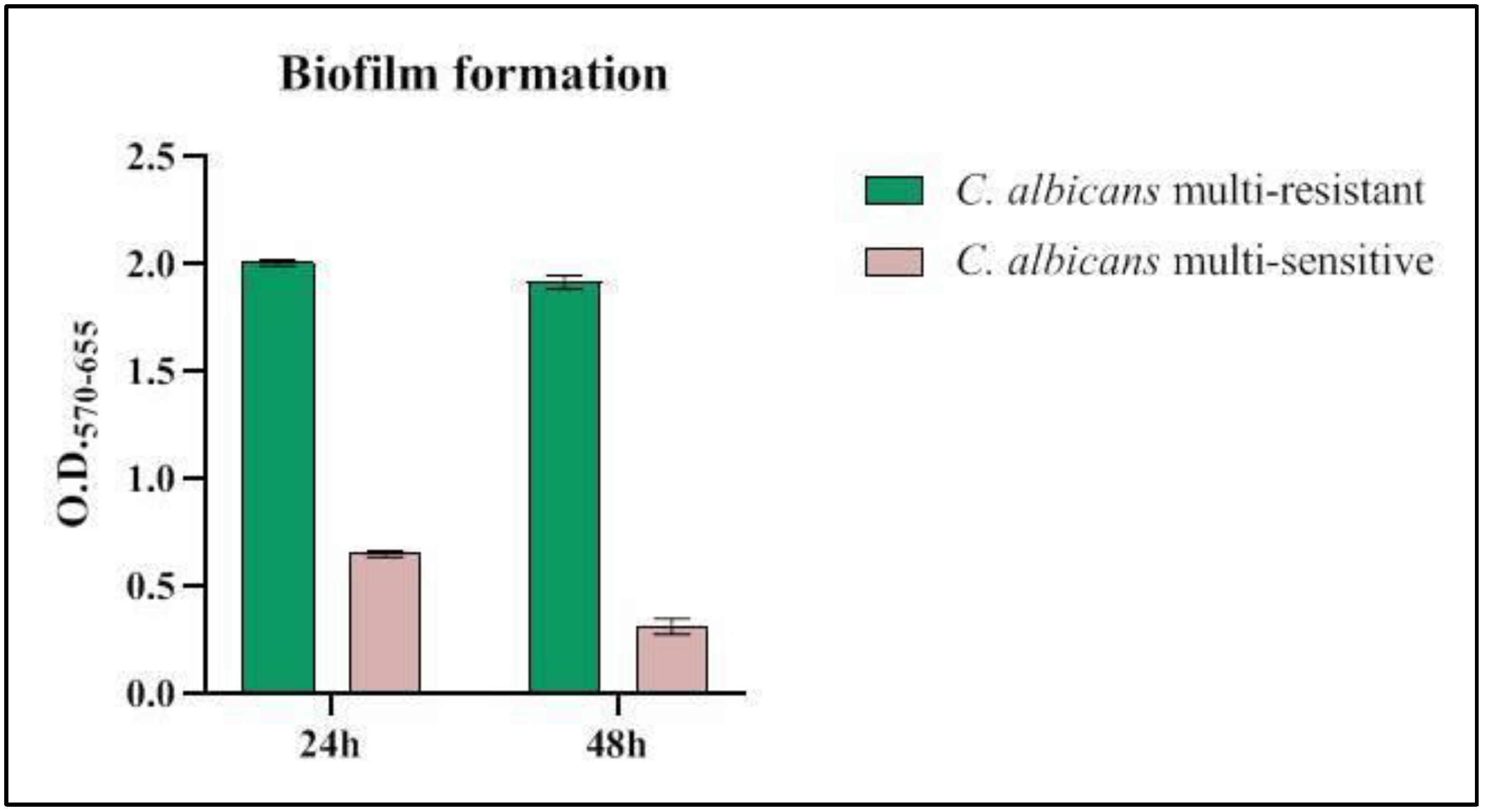
3. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Darwazeh, A.M.G.; Darwazeh, T.A. What Makes Oral Candidiasis Recurrent Infection? A Clinical View. J. Mycol. 2014, 2014, 758394. [Google Scholar] [CrossRef]
- Wen, S.-R.; Yang, Z.-H.; Dong, T.-X.; Li, Y.-Y.; Cao, Y.-K.; Kuang, Y.-Q.; Li, H.-B. Deep Fungal Infections Among General Hospital Inpatients in Southwestern China: A 5-Year Retrospective Study. Front. Public Health 2022, 10, 842434. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.; Rao, R.S.; Majumdar, B.; Anil, S. Clinical Appearance of Oral Candida Infection and Therapeutic Strategies. Front. Microbiol. 2015, 6, 1391. [Google Scholar] [CrossRef] [Green Version]
- Naik, B.; Ahmed, S.M.Q.; Laha, S.; Das, S.P. Genetic Susceptibility to Fungal Infections and Links to Human Ancestry. Front. Genet. 2021, 12, 709315. [Google Scholar] [CrossRef] [PubMed]
- Hamad, M.; Mohammad, M.G.; Abu-Elteen, K.H. Immunity to Human Fungal Infections. In Fungi Biology and Applications, 3rd ed.; Kavanagh, K., Ed.; John Wiley & Sons, Inc.: New York, NY, USA, 2017; pp. 275–298. [Google Scholar] [CrossRef]
- Deepa, A.; Nair, B.; Sivakumar, T.; Joseph, A. Uncommon opportunistic fungal infections of oral cavity: A review. J. Oral Maxillofac. Pathol. 2014, 18, 235–243. [Google Scholar] [CrossRef] [Green Version]
- Wawrysiuk, S.; Rechberger, T.; Futyma, K.; Miotła, P. Candida lusitaniae—A case report of an intraperitoneal infection. Menopausal Rev. 2018, 17, 94–96. [Google Scholar] [CrossRef]
- Raja, A.; Park, J. Disseminated Candida lusitaniae: Nosocomial Acquisition Secondary to an Indwelling Urinary Catheter. Case Rep. Infect. Dis. 2021, 2021, 6632730. [Google Scholar] [CrossRef]
- Apsemidou, A.; Füller, M.A.; Idelevich, E.A.; Kurzai, O.; Tragiannidis, A.; Groll, A.H. Candida lusitaniae Breakthrough Fungemia in an Immuno-Compromised Adolescent: Case Report and Review of the Literature. J. Fungi 2020, 6, 380. [Google Scholar] [CrossRef]
- Khan, Z.; Ahmad, S.; Al-Sweih, N.; Khan, S.; Joseph, L. Candida lusitaniae in Kuwait: Prevalence, antifungal susceptibility and role in neonatal fungemia. PLoS ONE 2019, 14, e0213532. [Google Scholar] [CrossRef] [Green Version]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J.; et al. Executive Summary: Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2016, 62, 409–417. [Google Scholar] [CrossRef] [Green Version]
- Cheng, F.-S.; Pan, D.; Chang, B.; Jiang, M.; Sang, L.-X. Probiotic mixture VSL#3: An overview of basic and clinical studies in chronic diseases. World J. Clin. Cases 2020, 8, 1361–1384. [Google Scholar] [CrossRef] [PubMed]
- Atriwal, T.; Azeem, K.; Husain, F.M.; Hussain, A.; Khan, M.N.; Alajmi, M.F.; Abid, M. Mechanistic Understanding of Candida albicans Biofilm Formation and Approaches for Its Inhibition. Front. Microbiol. 2021, 12, 638609. [Google Scholar] [CrossRef] [PubMed]
- Gulati, M.; Nobile, C.J. Candida albicans biofilms: Development, regulation, and molecular mechanisms. Microbes Infect. 2016, 18, 310–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panariello, B.H.D.; Klein, M.I.; Mima, E.G.D.O.; Pavarina, A.C. Fluconazole impacts the extracellular matrix of fluconazole-susceptible and -resistant Candida albicans and Candida glabrata biofilms. J. Oral Microbiol. 2018, 10, 1476644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, Q.; Ren, B.; Zhou, X.; Zhang, L.; Xu, X. Cross-kingdom interaction between Candida albicans and oral bacteria. Front. Microbiol. 2022, 13, 911623. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Liu, Y.; Benhamou, R.; Sanchez, H.; Simon-Soro, A.; Li, Y.; Hwang, G.; Fridman, M.; Andes, D.; Koo, H. Bacterial-derived exopolysaccharides enhance antifungal drug tolerance in a cross-kingdom oral biofilm. ISME J. 2018, 12, 1427–1442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arias, C.R.; Burns, J.K.; Friedrich, L.M.; Goodrich, R.M.; Parish, M.E. Yeast Species Associated with Orange Juice: Evaluation of Different Identification Methods. Appl. Environ. Microbiol. 2002, 68, 1955–1961. [Google Scholar] [CrossRef] [Green Version]
- Matsubara, V.H.; Wang, Y.; Bandara, H.M.H.N.; Mayer, M.P.A.; Samaranayake, L.P. Probiotic lactobacilli inhibit early stages of Candida albicans biofilm development by reducing their growth, cell adhesion, and filamentation. Appl. Microbiol. Biotechnol. 2016, 100, 6415–6426. [Google Scholar] [CrossRef] [Green Version]
- Krzyściak, W.; Kościelniak, D.; Papież, M.; Vyhouskaya, P.; Zagórska-Świeży, K.; Kołodziej, I.; Bystrowska, B.; Jurczak, A. Effect of a Lactobacillus Salivarius Probiotic on a Double-Species Streptococcus Mutans and Candida Albicans Caries Biofilm. Nutrients 2017, 9, 1242. [Google Scholar] [CrossRef] [Green Version]
- Contaldo, M.; Di Stasio, D.; Romano, A.; Fiori, F.; Della Vella, F.; Rupe, C.; Lajolo, C.; Petruzzi, M.; Serpico, R.; Lucchese, A. Oral candidiasis and novel therapeutic strategies: Antifungals, phytotherapy, probiotics, and photodynamic therapy. Curr. Drug Deliv. 2022, 20, 441–456. [Google Scholar] [CrossRef]
- Schlee, M.; Harder, J.; Köten, B.; Stange, E.F.; Wehkamp, J.; Fellermann, K. Probiotic lactobacilli and VSL#3 induce enterocyte β-defensin 2. Clin. Exp. Immunol. 2008, 151, 528–535. [Google Scholar] [CrossRef]
- Fusco, A.; Savio, V.; Donniacuo, M.; Perfetto, B.; Donnarumma, G. Antimicrobial Peptides Human Beta-Defensin-2 and -3 Protect the Gut During Candida albicans Infections Enhancing the Intestinal Barrier Integrity: In Vitro Study. Front. Cell. Infect. Microbiol. 2021, 11, 666900. [Google Scholar] [CrossRef] [PubMed]
- Perez-Rodriguez, A.; Eraso, E.; Quindós, G.; Mateo, E. Antimicrobial Peptides with Anti-Candida Activity. Int. J. Mol. Sci. 2022, 23, 9264. [Google Scholar] [CrossRef] [PubMed]
- Abirami, C.P.; Venugopal, P.V. Antifungal activity of three mouth rinses—In vitro study. Indian J. Pathol. Microbiol. 2005, 48, 43–44. [Google Scholar] [PubMed]
- Petersen, E.E.; Weissenbacher, E.R.; Hengst, P.; Spitzbart, H.; Wolfgang, W.; Wolff, F.; Dreher, E.; Ernst, U.; Della Casa, V.; Pohlig, G.; et al. Local treatment of vaginal infections of varying etiology with dequalinium chloride or povidone iodine. A randomised, double-blind, active-controlled, multicentric clinical study. Arzneimittelforschung 2002, 52, 706–715. [Google Scholar] [CrossRef]
- Yu, H.; Tak-Yin, M. The efficacy of povidone-iodine pessaries in a short, low-dose treatment regime on candidal, trichomonal and non-specific vaginitis. Postgrad. Med. J. 1993, 69, S58–S61. [Google Scholar] [PubMed]
- Bonowitz, A.; Schaller, M.; Laude, J.; Reimer, K.; Korting, H.C. Comparative Therapeutic and Toxic Effects of Different Povidone Iodine (PVP-I) Formulations in a Model of Oral Candidosis Based on in vitro Reconstituted Epithelium. J. Drug Target. 2001, 9, 75–83. [Google Scholar] [CrossRef]
- Berkowitz, R.J.; Hughes, C.; Rudnick, M.; Gordon, E.M.; Strandjord, S.; Cheung, N.K.; Warkentin, P.; Coccia, P.F. Oropharyngeal Candida prophylaxis in pediatric bone marrow transplant patients. J. Pediatr. Hematol. 1985, 7, 82–86. [Google Scholar]
- Kean, R.; McKloud, E.; Townsend, E.M.; Sherry, L.; Delaney, C.; Jones, B.L.; Williams, C.; Ramage, G. The comparative efficacy of antiseptics against Candida auris biofilms. Int. J. Antimicrob. Agents 2018, 52, 673–677. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antifungals | C. albicans | C. lusitaniae |
|---|---|---|
| 5-Flucytosine | 32 NI | ≤0.06 NI |
| Amphotericin B | >8 R | 1 S |
| Anidulafungin | >8 R | ≤0.015 S |
| Caspofungin | >8 R | 0.06 NI |
| Micafungin | >8 R | 0.015 S |
| Fluconazole | >256 R | 0.25 S |
| Itraconazole | >16 NI | 0.03 S |
| Posaconazole | >8 R | 0.03 S |
| Voriconazole | >8 R | ≤0.008 NI |
| Nystatin | >8 R | ≤0.06 NI |
| Antifungals | C. albicans Multi-Sensitive | C. albicans Multi-Resistant |
|---|---|---|
| 5-Flucytosine | ≤0.25 S | 32 NI |
| Amphotericin B | ≤1 S | >8 R |
| Anidulafungin | ≤0.25 S | >8 R |
| Caspofungin | ≤0.25 S | >8 R |
| Micafungin | ≤0.25 S | >8 R |
| Fluconazole | 0.25 S | >256 R |
| Itraconazole | ≤0.25 S | >16 NI |
| Posaconazole | ≤0.06 S | >8 R |
| Voriconazole | ≤0.12 S | >8 R |
| Nystatin | ≤0.25 S | >8 R |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fusco, A.; Contaldo, M.; Savio, V.; Baroni, A.; Ferraro, G.A.; Di Stasio, D.; Lucchese, A.; Chiaromonte, A.; Donnarumma, G.; Serpico, R. An Unconventional Oral Candidiasis in an Immunocompetent Patient. J. Fungi 2023, 9, 295. https://doi.org/10.3390/jof9030295
Fusco A, Contaldo M, Savio V, Baroni A, Ferraro GA, Di Stasio D, Lucchese A, Chiaromonte A, Donnarumma G, Serpico R. An Unconventional Oral Candidiasis in an Immunocompetent Patient. Journal of Fungi. 2023; 9(3):295. https://doi.org/10.3390/jof9030295
Chicago/Turabian StyleFusco, Alessandra, Maria Contaldo, Vittoria Savio, Adone Baroni, Giuseppe A. Ferraro, Dario Di Stasio, Alberta Lucchese, Adriana Chiaromonte, Giovanna Donnarumma, and Rosario Serpico. 2023. "An Unconventional Oral Candidiasis in an Immunocompetent Patient" Journal of Fungi 9, no. 3: 295. https://doi.org/10.3390/jof9030295