

Abbreviated Mental Test Score (AMTS) - Department of Health
Abbreviated Mental Test Score (AMTS) - Department of Health
Abbreviated Mental Test Score (AMTS) - Department of Health

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
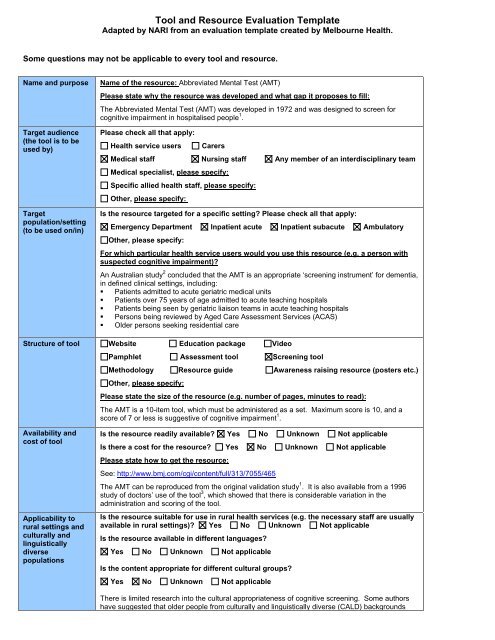
Tool and Resource Evaluation Template<br />
Adapted by NARI from an evaluation template created by Melbourne <strong>Health</strong>.<br />
Some questions may not be applicable to every tool and resource.<br />
Name and purpose Name <strong>of</strong> the resource: <strong>Abbreviated</strong> <strong>Mental</strong> <strong>Test</strong> (AMT)<br />
Target audience<br />
(the tool is to be<br />
used by)<br />
Target<br />
population/setting<br />
(to be used on/in)<br />
Please state why the resource was developed and what gap it proposes to fill:<br />
The <strong>Abbreviated</strong> <strong>Mental</strong> <strong>Test</strong> (AMT) was developed in 1972 and was designed to screen for<br />
cognitive impairment in hospitalised people 1 .<br />
Please check all that apply:<br />
<strong>Health</strong> service users Carers<br />
Medical staff Nursing staff Any member <strong>of</strong> an interdisciplinary team<br />
Medical specialist, please specify:<br />
Specific allied health staff, please specify:<br />
Other, please specify:<br />
Is the resource targeted for a specific setting? Please check all that apply:<br />
Emergency <strong>Department</strong> Inpatient acute Inpatient subacute Ambulatory<br />
Other, please specify:<br />
For which particular health service users would you use this resource (e.g. a person with<br />
suspected cognitive impairment)?<br />
An Australian study 2 concluded that the AMT is an appropriate ‘screening instrument’ for dementia,<br />
in defined clinical settings, including:<br />
� Patients admitted to acute geriatric medical units<br />
� Patients over 75 years <strong>of</strong> age admitted to acute teaching hospitals<br />
� Patients being seen by geriatric liaison teams in acute teaching hospitals<br />
� Persons being reviewed by Aged Care Assessment Services (ACAS)<br />
� Older persons seeking residential care<br />
Structure <strong>of</strong> tool Website Education package Video<br />
Availability and<br />
cost <strong>of</strong> tool<br />
Applicability to<br />
rural settings and<br />
culturally and<br />
linguistically<br />
diverse<br />
populations<br />
Pamphlet Assessment tool Screening tool<br />
Methodology Resource guide Awareness raising resource (posters etc.)<br />
Other, please specify:<br />
Please state the size <strong>of</strong> the resource (e.g. number <strong>of</strong> pages, minutes to read):<br />
The AMT is a 10-item tool, which must be administered as a set. Maximum score is 10, and a<br />
score <strong>of</strong> 7 or less is suggestive <strong>of</strong> cognitive impairment 1 .<br />
Is the resource readily available? Yes No Unknown Not applicable<br />
Is there a cost for the resource? Yes No Unknown Not applicable<br />
Please state how to get the resource:<br />
See: http://www.bmj.com/cgi/content/full/313/7055/465<br />
The AMT can be reproduced from the original validation study 1 . It is also available from a 1996<br />
study <strong>of</strong> doctors’ use <strong>of</strong> the tool 3 , which showed that there is considerable variation in the<br />
administration and scoring <strong>of</strong> the tool.<br />
Is the resource suitable for use in rural health services (e.g. the necessary staff are usually<br />
available in rural settings)? Yes No Unknown Not applicable<br />
Is the resource available in different languages?<br />
Yes No Unknown Not applicable<br />
Is the content appropriate for different cultural groups?<br />
Yes No Unknown Not applicable<br />
There is limited research into the cultural appropriateness <strong>of</strong> cognitive screening. Some authors<br />
have suggested that older people from culturally and linguistically diverse (CALD) backgrounds
Person-centred<br />
principles<br />
Training<br />
requirements<br />
Administration<br />
details<br />
Data collection and<br />
analysis<br />
Sensitivity and<br />
specificity<br />
Face Validity<br />
Reliability<br />
have poorer ‘test-taking’ skills and may experience greater anxiety about cognitive assessment.<br />
Others conclude that although cultural bias is common in screening tests for cognition, sensitive<br />
administration and interpretation <strong>of</strong> results can minimise the effects 4-6 .<br />
There are questions in the AMT which are not necessarily appropriate to CALD groups – e.g. ‘date<br />
<strong>of</strong> First World War’ may vary according to your country <strong>of</strong> origin and may be a less significant event<br />
for people <strong>of</strong> non-European background; similarly ‘name <strong>of</strong> the current monarch’ may be affected<br />
by cultural background.<br />
However modified/culturally-adapted versions do exist, which show good sensitivity and specificity.<br />
The issue is that adapting a tool can significantly change it’s performance and validation studies<br />
need to be conducted within the target population on new versions. 7<br />
Does the resource adhere to/promote person-centred health care?<br />
Yes No Unknown Not applicable<br />
Cognitive screening instruments have been criticised for failing to take into account educational<br />
level, cultural background, literacy, and pr<strong>of</strong>iciency in English; which would suggest they are not<br />
person-centred tools. However, it could be argued that without an assessment <strong>of</strong> cognitive status<br />
patients/clients cannot be provided with care that is designed to meet their needs.<br />
It is important that administration <strong>of</strong> all cognitive assessment instruments is performed by a person<br />
trained in their use, and who is cognisant <strong>of</strong> their shortcomings; and that interpreters and patient<br />
liaison staff are utilised as necessary.<br />
Is additional training necessary to use the resource?<br />
Yes No Unknown Not applicable<br />
If applicable, please state how extensive any training is, and what resources are required:<br />
Whilst no formal training is required to use this instrument, it is advisable that users are familiar<br />
with the tool and the process for administration, in order to produce reliable results.<br />
How long does the resource take to use? 0-5 mins 5-15 mins 15-25mins 25mins<br />
Can the resource be used as a standalone, or must it be used in conjunction with other<br />
tools, resources, and procedures?<br />
Standalone<br />
Must be used with other resources, please specify:<br />
Can be used with other tools, please specify:<br />
Are additional resources required to collect and analyse data from the resource?<br />
Yes No Unknown Not applicable<br />
If applicable, please state any special resources required (e.g. computer s<strong>of</strong>tware):<br />
Sensitivity is the proportion <strong>of</strong> people that will be correctly identified by the tool.<br />
Specificity is the probability that an individual who does not have the condition being tested<br />
for will be correctly identified as negative.<br />
Has the sensitivity and specificity <strong>of</strong> the resource been reported?<br />
Yes No Unknown Not applicable<br />
If applicable, please state what has been reported:<br />
A cut-<strong>of</strong>f score <strong>of</strong> 7 and 8 provides the greatest sensitivity and specificity 8 .<br />
It is important to note that changing the questions and/or omitting certain questions – an apparently<br />
common practice – will affect the reliability, validity, and sensitivity <strong>of</strong> the AMT 3 .<br />
There is some evidence to suggest that the AMT can be used to identify post-operative delirium, in<br />
those aged 65+, if the tool is administered to patients on the day before and third day after their<br />
surgery 9 . A decline <strong>of</strong> 2 or more points in AMT score post-operatively is suggestive <strong>of</strong> delirium<br />
(sensitivity 93%; specificity 84%).<br />
Does the resource appear to meet the intended purpose?<br />
Yes No Unknown Not applicable<br />
Correlates well with other cognitive assessment tools 10<br />
Reliability is the extent to which the tool’s measurements remain consistent over repeated<br />
tests <strong>of</strong> the same subject under identical conditions. Inter-rater reliability measures<br />
whether independent assessors will give similar scores under similar conditions.
Strengths<br />
Limitations<br />
References and<br />
further reading<br />
Has the reliability <strong>of</strong> the resource been reported?<br />
Yes No Unknown Not applicable<br />
If applicable, please state what has been reported:<br />
The AMT has been shown to correlate well with other measures <strong>of</strong> cognition and can reliably rule<br />
out dementia (but does not diagnose it) 2,10 ; it also demonstrates high internal consistency 8 . The<br />
AMT has been shown to be a more reliable indicator <strong>of</strong> cognitive impairment than clinical judgment<br />
for patients who score in the mid-range 11<br />
What are the strengths <strong>of</strong> the resource? Is the resource easy to understand and use? Are<br />
instructions provided on how to use the resource? Is the resource visually well presented<br />
(images, colour, font type/ size)? Does the resource use older friendly terminology (where<br />
relevant), avoiding jargon?<br />
Please state any other known strengths, using dot points:<br />
• Patients do not have to read, write, or draw anything to complete test, and so completion<br />
<strong>of</strong> the AMT is not affected by visual impairment, which is a common problem in older<br />
people.<br />
• The AMT is quick and simple to use and is a more reliable indicator <strong>of</strong> cognitive<br />
impairment than clinical judgment for scores in the mid-range.<br />
What are the limitations <strong>of</strong> the tool/resource? Is the tool/resource difficult to understand<br />
and use? Are instructions provided on how to use the tool/resource? Is the tool/resource<br />
poorly presented (images, colour, font type/ size)? Does the tool/resource use difficult to<br />
understand jargon?<br />
Please state any other known limitations, using dot points:<br />
• Certain items such as ‘name <strong>of</strong> the monarch’ and ‘date <strong>of</strong> First World War’ are potentially<br />
less appropriate than they were when the AMT was developed, and this may affect its<br />
validity.<br />
Supporting references and associated reading.<br />
1. Hodkinson HM. Evaluation <strong>of</strong> a mental test score for assessment <strong>of</strong> mental impairment in<br />
the elderly. Age & Ageing, 1972;1(4):233-8.<br />
2. Flicker L, LoGiudice D, Carlin JB, Ames D. The predictive value <strong>of</strong> dementia screening<br />
instruments in clinical populations. International Journal <strong>of</strong> Geriatric Psychiatry,<br />
1997;12(2):203-9.<br />
3. Holmes J, Gilbody S. Differences in use <strong>of</strong> abbreviated mental test score by geriatricians<br />
and psychiatrists. BMJ, 1996;313(7055):465-.<br />
4. Parker C, Philp I, Sarai M, Rauf A. Cognitive screening for people from minority ethnic<br />
backgrounds. Nursing Older People, 2007;18(12):31-6.<br />
5. Chiu HFK, Lam LCW. Relevance <strong>of</strong> outcome measures in different cultural groups - does<br />
one size fit all? International Psychogeriatrics, 2007;19(3):457-66.<br />
6. Lydall-Smith S, Moorhouse B. Culturally Approriate Dementia Assessment. Centre for<br />
Applied Gerontology, Bundoora Extended Care Centre, Victora. 1995.<br />
7. Parker C, Philp I. Screening for cognitive impairment among older people in black and<br />
minority ethnic groups. Age & Ageing, 2004;33(5):447-52.<br />
8. Jitapunkul S, Pillay I, Ebrahim S. The abbreviated mental test: its use and validity. Age &<br />
Ageing., 1991;20(5):332-6.<br />
9. Ni Chonchubhair A, Valacio R, Kelly J, O'Keefe S. Use <strong>of</strong> the abbreviated mental test to<br />
detect postoperative delirium in elderly people. British Journal <strong>of</strong> Anaesthesia,<br />
1995;75(4):481-2.<br />
10. Antonelli Incalzi R, Cesari M, Pedone C, Carosella L, Carbonin PU, Gruppo Italiano di<br />
Farmacovigilanza nell'Anziano. Construct validity <strong>of</strong> the abbreviated mental test in older<br />
medical inpatients. Dementia & Geriatric Cognitive Disorders., 2003;15(4):199-206.<br />
11. Burleigh E, Reeves I, McAlpine C, Davie J. Can doctors predict patients' abbreviated<br />
mental test scores? Age and Ageing, 2002;31(4):303-306.














